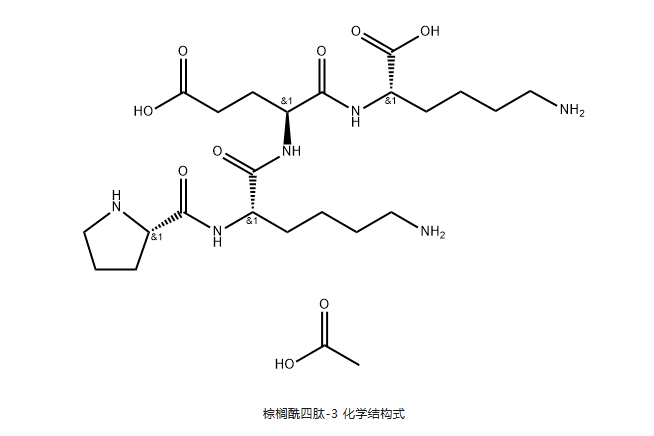
palmitoyl tetrapeptide -3(Palmitoyl Tetrapeptide-3), also known as palmitoyl tetrapeptide -7, its amino acid sequence is Pal-Gly-Gln-Pro-Arg, abbreviated as Pal-GQPR, which belongs to one of the palmitoyl oligopeptide series polypeptides in the signal class peptide.
palmitoyl series of peptides belong to signal peptides, which can promote the synthesis of matrix protein, especially collagen, and may also promote the generation of elastin, hyaluronic acid, glycosaminoglycan, fibronectin and other proteins. Palmitoyl peptides promote collagen synthesis by increasing the activity of stromal cells, increasing skin elasticity and more youthful appearance. Similar to traditional anti-wrinkle raw materials, such as vitamin C and vitamin A derivatives, but the ability to promote collagen production is far better than vitamin C and vitamin A retinol. At present, there are many synthetic schemes for palmitoyl pentapeptide -3 and palmitoyl tripeptide -1 in the world, while palmitoyl tetrapeptide -3 is very few.
basic information
Chinese Name: Palmitoyl Tetrapeptide -3
English name: Palmitoyl Tetrapeptide-3
Company No.: GT-C006
CAS No.: 221227-05-0
sequence: Pal-GQPR
molecular formula: C34H62N8O7
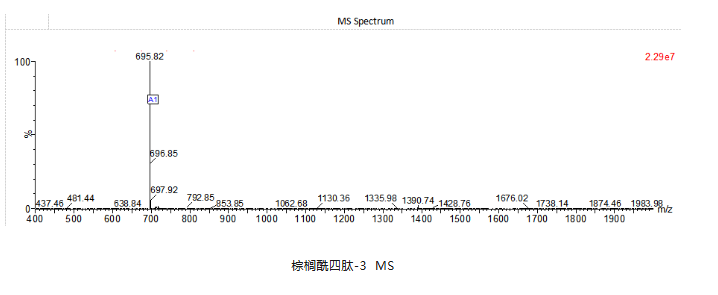
molecular weight: 694.92
Synthesis method
(1) resin activation: 10g 2-CTC-Resin resin (Lot No:GRAS1014-1,Cross-linking:1% DVB,ParticleSize:100-200mesh,Substitution 1.75mmol/g) is added into a reactor, 80mL DCM is added, stirred and soaked at room temperature for 10min to fully swell and activate.
(2) Synthesis of Fmoc-Arg(pbf)-2-CTC Resin Peptide Resin: 12.49gFmoc-Arg(pbf)-OH, 12mL DIEA and 100mL DCM are added to the resin in step (1), and the reaction is stirred at room temperature for 2h, wherein the molar ratio of 2-CTC Resin, Fmoc-Arg(pbf)-OH and DIEA is 1: 1.1: 4, and 90mL DMF and 90mL are washed twice respectively, A protected peptide resin was obtained.
(3) A solution of 20% piperidine 100mL DMF was added to the resin peptide in step (2), and the reaction was stirred at room temperature for 20min. The solution was removed by suction filtration, a solution 100mL 20% piperidine in DMF was added again, and the reaction was stirred at room temperature for 10min to remove the 9-fluorenylmethoxycarbonyl group on 2-CTC Resin. Wash twice with 100mL of isopropanol and 100mL mL of DMF.
(4) Synthesis of Pro-Arg(pbf)-2-CTC Resin Peptide Resin: Fmoc-Pro-OH(11.8g), HOBT(7.09g), DIC(8.2mL) and DMF(90mL) are added to the resin in step (3), and the reaction is stirred at room temperature for 2h, wherein the molar ratio of 2-CTC-Resin, Fmoc-Pro-OH, HOBT and DIC is 1: 2: 3: 3, washing was performed twice each with 90mL of isopropanol and 100mL mL of DMF to obtain a protected peptide resin.
(5) Synthesis of Gly-Gln(trt)-Pro-Arg(pbf)-2-CTC Resin Peptide Resin: Steps (3) and (4) were repeated, and FmocGln(trt)-OH and Fmoc-Gly-OH were successively ligated to obtain Gly-Gln(trt)-ProArg(pbf)-2-CTC Resin peptide resin.
(6) Synthesis of Pal-Gly-Gln(trt)-Pro-Arg(pbf)-2-CTC Resin Peptide Resin: 10.7mL of palmitoyl chloride, 7.24mL mL of DIEA and 120mL mL of DCM were added to the resin in step (4), and the reaction was stirred at room temperature for 20min. Wherein, the molar ratio of 2-CTC Resin, palmitoyl chloride and DIEA is 1: 2: 2.5, washed twice with 120mL isopropanol and 120mL mL DMF respectively, washed three times with methanol, and dried to obtain 24g of resin peptide.
(7) Preparation of palmitoyl tetrapeptide-3 Preparation of peptide resin cutting solution: Triisopropylsilane, trifluoroacetic acid, thioanisole and water are added into a beaker in a volume ratio of 5: 4: 88: 3 and stirred for mixing.
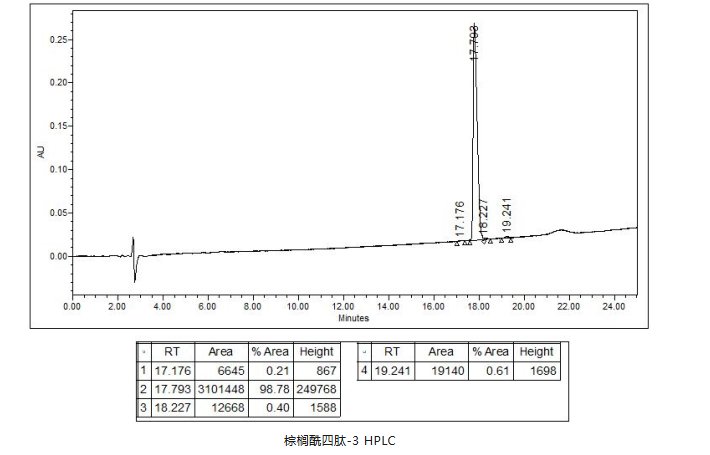
(8) Cleavage of peptide resin: 200mL of cutting liquid is added to the peptide resin in step (6), stirred and reacted at room temperature for 2h, filtered, the filtrate is concentrated to oily substance at 38 ℃, poured into frozen 400mL of anhydrous ether, 1.5mL of concentrated hydrochloric acid is added dropwise, a large amount of white solid is precipitated, stirred, centrifuged, supernatant is separated, and dried under reduced pressure at room temperature to obtain crude palmitoyl tetrapeptide -3, after purification by reversed-phase chromatography, concentration and freeze-drying, 11.75g of pure palmitoyl tetrapeptide -3 was obtained, and the purity was> 98%.
Post time: 2026-07-23